01Care-Gap Detection & Closure
Every care gap, surfaced and ranked to close.
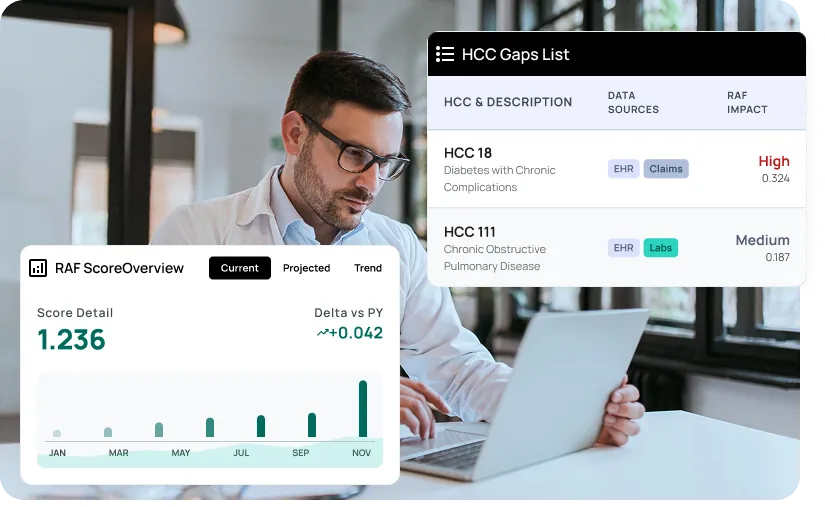
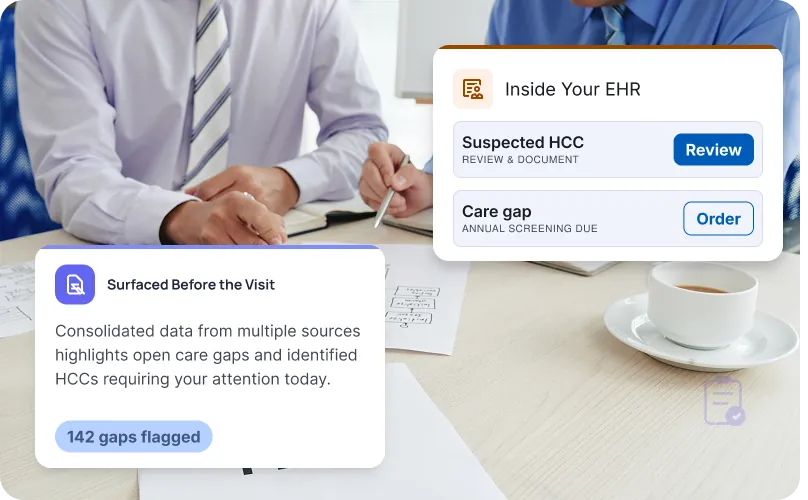
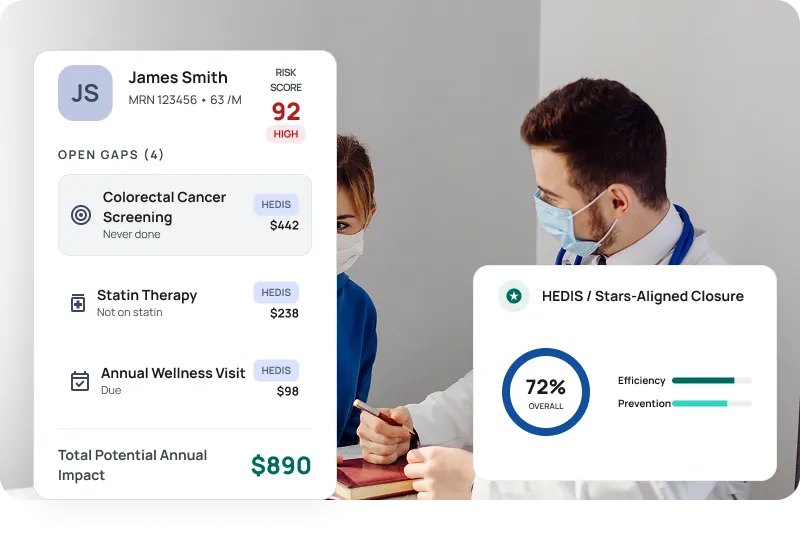
Detect open quality and care gaps per patient, panel, and measure, prioritize them by clinical urgency and revenue impact, and drive closure through daily-refreshed worklists.
- Quality and care gaps detected per patient, panel, and measure
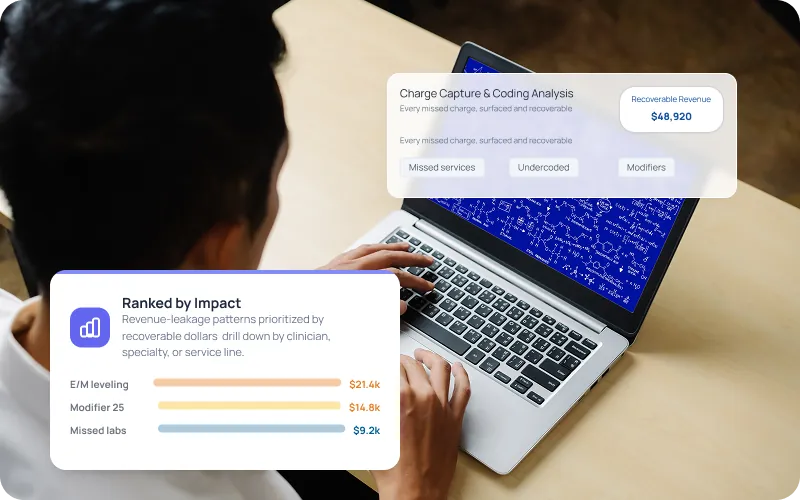
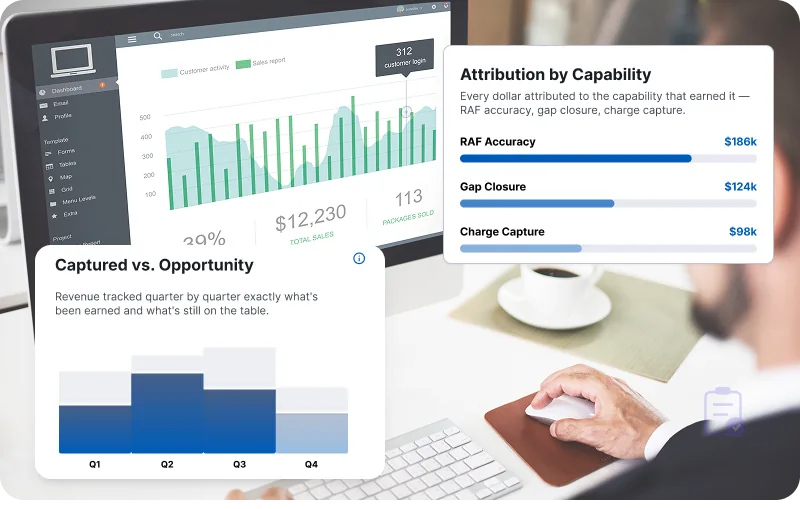
- Prioritization by clinical urgency and revenue impact
- Daily-refreshed gap-closure worklists
- Outreach and recall lists for open-gap patients
- Clinician huddle and call-center feeds
- HEDIS / Stars-aligned measure closure